A friend recently emailed me a link to a doctor’s autobiographical piece on the state of poverty medicine, which discusses questions that are critical even and especially in the aftermath of the ACA. Rachel Pearson’s Texas’ Other Death Penalty: A Galveston Medical Student Describes Life and Death in the So-Called Safety Net provides an account of some of the struggles that health care professionals, patients, and their loved ones have to deal with as they bring their diseases to bear on US health care systems.
Throughout the article, Pearson articulates the mottoes that are (or have been) part of her journey as a medical-doctor-in-training. The mottoes are worth further reflection as part of thinking about what it means to treat and heal people.
- University of Texas Medical Branch had this as its motto: “Here for the Health of Texas” before switching to this: “Working together to work wonders.” Interesting that the focus shifts away from an outward-looking focus on Texas’ health (open, ostensibly, to whomever) toward an inward-looking staff-driven motto. The question of care looms a bit. Wonders for whom? Pearson not-so-subtly suggests that UTMB’s wonders are specifically for people who can pay, especially medical tourists.
This isn’t only Texas, of course. Texas here stands as an example of what I think has come to be quintessentially American medicine.
On the first day of class, I ask my students how they would describe health care ethics. Most of them raise themes that would be familiar to most of us because they’re the issues in the news: abortion, stem-cell research, genetic testing, IVF and euthanasia. Almost no one mentions poverty. But of the course of the semester, through meetings with doctors and through their own service work at the area’s free clinics, my students begin to see that health care ethics is about far more than these issues. Indeed, most of the issues they thought were issues are, in reality, dealt with relatively little by the OB-GYNs, pediatricians, psychiatrists, family care practitioners, nurses and physical therapists that they meet.
IVF, it turns out, is something accessible to only a very small, relatively rich portion of the population. Ditto genetic testing, ditto many of the cool new drugs that treat bad diseases and the technologies that can be used to diagnose them. But the conversation focuses on those.
In the place of those issues, students encounter instead the chronic asthma patient and her mother – the girl whose condition is quite treatable but ends up each month incurring hospital bills that are far more expensive than the drugs used to treat asthma. That’s in part because her mother has a low-wage job and no car, so takes the bus, which only runs once an hour and shuts down early in the evening due to transportation cut backs. That makes it more difficult not only to get to work in a timely manner, but to make it to a pharmacy, a free clinic, or a regular doctor check up that would be cheaper than hospitalization. Then my students discover that part of the reason for the girl’s chronic asthma is that they live in an apartment building they can afford, but which is prone to mold and other allergens, and is a spot with a high level of smoking, which aggravates the condition.
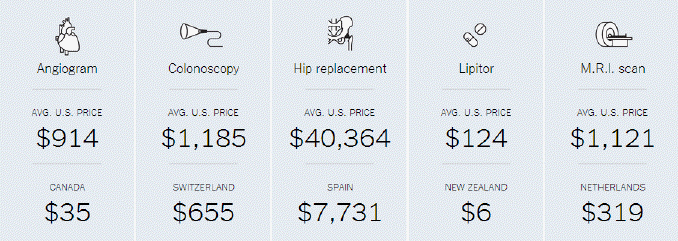
I also emphasize the vast disparity in costs of very common treatments in the US compared to some other nations. For example:
Students quickly grasp the intricacy of the questions and pretty readily see that there are a host of problems that aren’t easily fixable. Health care ethics on the ground becomes about the issues that aren’t in the news.
The issues that make the news, however, are the questions that we ask when we’ve got money. Benedict XVI observed in Caritas in Veritate (22): “On the part of rich countries there is excessive zeal for protecting knowledge through an unduly rigid assertion of the right to intellectual property, especially in the field of health care.” One of his concerns is the ways in which health care is seen as a commodity to be distributed among those who can pay… but that is not the way that health care operates. The mottoes highlighted by Pearson, however, seem to suggest a shift from seeing health care as part of a basic human right, to seeing health care as a commodity.
- St. Vincent’s House, where Pearson has volunteered, has the motto: “An oasis of hope, expecting miracles.” A corollary quote is offered by one of Pearson’s med school professors: “A physician never takes away hope.”
But in a world where whatever hope a physician might offer is taken away by others not necessarily associated with the principals involved, those mottoes seem poignant for the fact that hope dies often, and expected miracles are rather infrequent. The free clinic is hosted by St. Vincent’s, Pearson explains. But the city has yet to rebuild public housing after Hurricane Ike…leaving the neighborhood in great disrepair. Pearson observes: “Just like the medical system, the city knows whose lives matter.” It isn’t the people living in those neighborhoods.
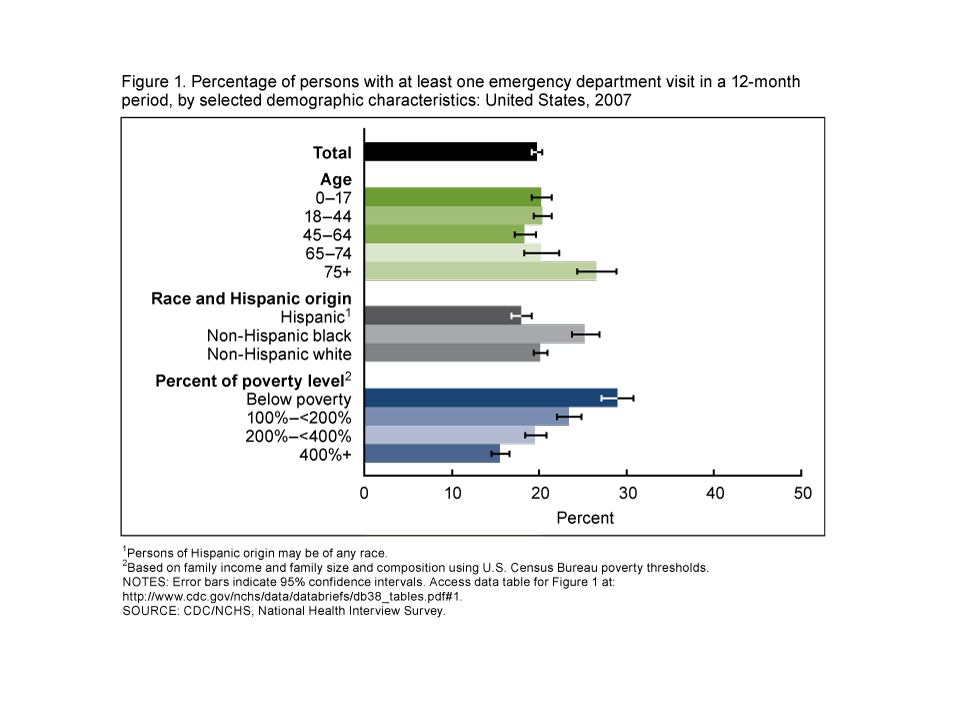
Pearson explains the myth about emergency care: that we think pretty much anybody can go to the ER and get the care they need and if they’re really in need, not have to pay for it. But that’s not true – patients get charged and bills get sent to collection agencies.
But more to the point, how many of these treatable diseases need to come under the category of “Needs a Miracle?” The ER hasn’t been designed or envisioned as a place for the kinds of treatable diseases that are present, though it clearly is responsible for treating more people at or below the poverty level.
ER medicine is more costly than preventative care as Reuters reports here:
For instance, at a program in Akron, Ohio, profiled in the new report, physicians and others coordinate care for patients with Type 2 diabetes. It reduced the average cost of care by more than 10 percent, or $3,185 per year, largely by reducing pricey emergency-room visits.
(See here for a link to a further discussion from Harvard Public Health)
Contrary to common belief, treatable diseases that are not true “emergencies” can’t fully be treated in the ER. Medical care of treatable diseases that don’t manifest themselves as emergencies are not going to receive the kind of care that they need. Pearson gives the example of her first patient at St. Vincent’s – a patient who probably had liver cancer, but for whom any diagnosable medical tests were far beyond reach in terms of economic and medical resources.
Pearson laments the treatable conditions that never get treated. It’s a question I post to my students too: the miracles we support and marvel at in terms of technological advances are not really getting at the belly of the beast.
Such a conundrum provides precisely the kind of example that church teaching decries. Again citing Benedict XVI in Caritas in Veritate (43)
A link has often been noted between claims to a “right to excess”, and even to transgression and vice, within affluent societies, and the lack of food, drinkable water, basic instruction and elementary health care in areas of the underdeveloped world and on the outskirts of large metropolitan centres.
What kind of rights to excess exist in our contemporary medical system? I would suggest that the “right to insurance” as mandated by the Affordable Care Act does little to mitigate against the kind of situations that Pearson discusses, since the people she narrates are precisely the people who fall into the gaps… not eligible for Medicaid, and exchanges in insurance too expensive.
Indeed, as commenter Norman Solomon notes at Common Dreams: Building Progressive Community:
The ACA is so complicated because it has been so relentlessly written for the benefit of—and largely written by—insurance companies….Obamacare is a mess largely because it builds a revamped healthcare system around the retrenched and extended power of insurance companies—setting back prospects for real healthcare reform for a decade or more. Egged on by corporate media and corporate politicians, much of the public will blame higher premiums on government intervention and not on the greedy insurance companies which, along with Big Pharma, helped write the law in the Obama White House and on Capitol Hill.
Ultimately the ones who lose will be the ones who slip through the cracks, like the million Texans not eligible for Medicaid, but also unable to pay for insurance, and who will continue to lose out in relation to some of the law’s “good parts” such as free preventative care check ups. And I think Solomon’s right: the winners will be the insurance companies, who are making money having to charge more for the insurance plans the law mandates that include much of what ought to count as basic health care: routine, and cost-effective, screenings for routine, treatable diseases when they’re caught early (e.g. routine physicals, colonscopies, etc.)
I think that in the midst of the rightful uproar over the ACA and its insurance mandate, we’ve totally lost the thread of conversation that Americans across the spectrum agree on: the health care system is broken. As someone who tends to identify socially Left, I think a single-payer health care system would best meet the kinds of concerns in Catholic teaching. But I want to hear that conversation from my friends on the Right. But we aren’t having those conversations, indeed, we’ve stopped having them, because we’ve been arguing about the ACA.
In addition, CV’s “right to excess” question about wealth disparity and health care is exactly one of the reasons why I tell my students about less-well known medical issues and advances, ones that are far less well-known than their more expensive counterparts. How about postage stamp-sized diagnostic medical tests, which are able to be xeroxed and copied for multitudes of populations who do not have access to ultrasound equipment or other expensive diagnostic tools? Or the $25 artificial knee and $400 hospital lamp for infants with jaundice created by a doctor with an interest in medical devices made affordable for people who live on $2 or less per day?
These, I think are the kinds of miracles that we need more of.
Now as the director of the free clinic, Pearson describes the frustration of “sending faxes into the abyss.” That’s the new motto for her, the one that indicates how little is able to be done, given our present political, economic and medical emphases. In the present situation, the real miracle and motto might be to “focus on treatable diseases that go untreated because of income gaps”.



{kind=link}